
When you're over 65 and taking medication for high blood pressure, one of the quietest dangers isn't the high number on the monitor-it's what happens when you stand up. A sudden dizzy spell, a blackout, a fall. These aren't just accidents. They're often tied to a condition called orthostatic hypotension-a sharp drop in blood pressure when you rise from sitting or lying down. And while many assume that lowering blood pressure too much causes this, the truth is more complex-and more hopeful.
What Is Orthostatic Hypotension, Really?
Orthostatic hypotension (OH) isn't just feeling lightheaded. It's a measurable drop: at least 20 mm Hg in systolic pressure or 10 mm Hg in diastolic pressure within three minutes of standing. It's not rare. In older adults with high blood pressure, it shows up in 3% to 26% of cases, according to data from the European Society of Cardiology. That’s one in four seniors. And it’s not just about age. As we get older, our bodies lose the ability to quickly adjust blood flow. The baroreflex-the body’s natural pressure regulator-slows down. Blood vessels don’t tighten as fast. The heart doesn’t pump as hard or as efficiently. These changes make standing up risky, especially if you’re on medication designed to lower blood pressure.But here’s the twist: treating high blood pressure aggressively doesn’t make OH worse. In fact, it might help. The landmark SPRINT trial and nine other studies involving over 18,000 people showed that people who aimed for a systolic pressure below 120 mm Hg had lower rates of orthostatic hypotension than those targeting 140 mm Hg. The risk didn’t go up-it went down by 17%. This flips the old belief that more aggressive treatment = more dizziness. The real problem isn’t the treatment. It’s the wrong drugs.
Which Medications Are Riskiest?
Not all blood pressure pills are created equal when it comes to OH. Some are far more likely to trigger dizziness and falls. Here’s what the data says:- Alpha blockers (like doxazosin, terazosin): Highest risk. Up to 28% of older adults on these develop OH. They relax blood vessels too much, too fast.
- Beta-blockers (like metoprolol, atenolol): Double the risk of sustained OH. They slow the heart and reduce its ability to respond to standing.
- Diuretics (water pills): Cause fluid loss, which lowers blood volume. A common culprit in dizziness after meals or bathroom trips.
- Central sympatholytics (like clonidine): Reduce nerve signals that help maintain blood pressure. High OH risk, especially at night.
- Calcium channel blockers: Mixed bag. Amlodipine and lacidipine are much safer-slow, steady action. Diltiazem and verapamil? Higher risk because older livers process them differently, leading to stronger effects.
- ACE inhibitors and ARBs (like lisinopril, losartan): Lowest risk. Studies show they may even protect against OH. Their mechanism helps maintain vascular tone without sudden drops.
One study found that switching from an alpha blocker to an ARB led to a 65% drop in dizziness and falls among elderly patients. That’s not a coincidence-it’s a clinical win.
Why More Intensive Treatment Is Safer Than You Think
It’s counterintuitive. If your blood pressure is already low when standing, why lower it further? Because the danger isn’t the standing pressure-it’s the supine pressure. If your blood pressure stays too high while lying down, it strains your heart and arteries. That’s what leads to strokes and heart attacks. Dr. Harry Goldblatt from Case Western Reserve University put it bluntly: "The impetus of adverse events in hypertensive patients with OH is supine/seated hypertension, not the standing BP."The American Heart Association says it plainly: don’t routinely stop or reduce blood pressure meds just because someone has OH-especially if they’re asymptomatic. The risk of stroke or heart failure from uncontrolled hypertension far outweighs the risk of occasional dizziness. The goal isn’t to avoid OH at all costs. It’s to avoid dangerous OH while keeping the heart protected.
What to Do: A Practical Step-by-Step Approach
If you or a loved one is over 65 and on blood pressure meds, here’s what actually works:- Review every medication. Ask your doctor: "Which of these could be causing dizziness?" Get rid of alpha blockers first. Then consider beta-blockers and diuretics if they’re not essential.
- Switch to safer alternatives. ACE inhibitors or ARBs are the first-line choice for older adults with OH risk. Amlodipine is a better calcium channel blocker than diltiazem.
- Time your doses. If you’re on a long-acting pill, take it no earlier than 3 hours before bed. This avoids nighttime drops that lead to morning dizziness.
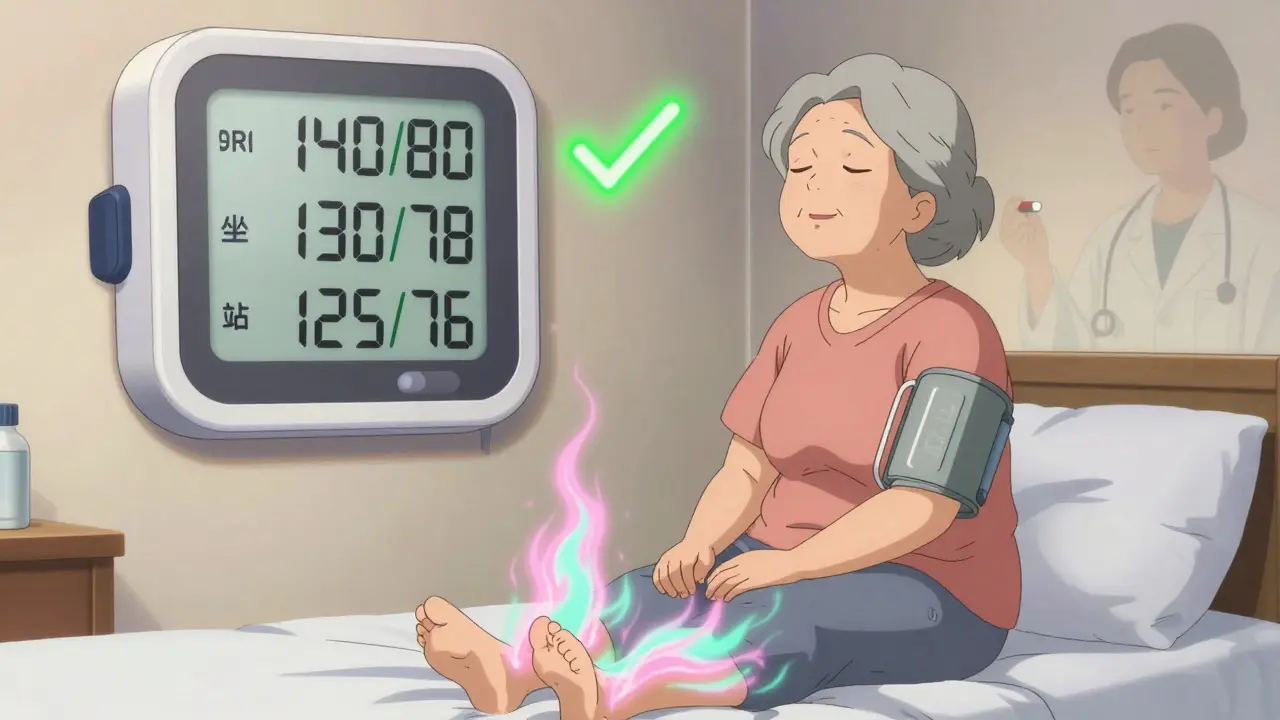
- Measure your blood pressure properly. Don’t just check it lying down. Take readings in three positions: lying, sitting, standing. Do this after sitting for 5 minutes, then again after standing for 1 and 3 minutes. This is the only way to catch OH.
- Don’t rush. Switching meds takes 4-6 weeks. Monitor BP closely. Don’t stop or change anything without supervision.
Non-Medication Fixes That Work
Medication isn’t the whole story. Simple habits can cut OH episodes by half:- Stand up slowly. Sit on the edge of the bed for a full minute before standing. Do this after naps, after meals, and after using the bathroom.
- Hydrate. Drink 16 oz of water 30 minutes before standing. It boosts blood volume and helps your body respond.
- Wear compression stockings. Not just for varicose veins. These help push blood back to the heart when standing.
- Elevate the head of your bed. Raise it 6-10 inches. This reduces nighttime fluid shifts and morning dizziness.
- Move your legs. Before standing, wiggle your toes, flex your calves. This activates your muscle pump and gets blood flowing.
Most people see improvement within 2-4 weeks of consistent practice. No pills needed.
What About Medications Just for OH?
Drugs like midodrine, droxidopa, or fludrocortisone exist-but they’re not first-line. They’re for severe, disabling cases where lifestyle changes and safer antihypertensives haven’t worked. These meds raise blood pressure, which sounds good-but they can spike supine pressure and cause headaches or strokes if not monitored. They’re a last resort, not a solution.The Bigger Picture: Why This Matters Now
In the U.S., over 74 million adults over 65 have high blood pressure. An estimated 2-19 million of them also have orthostatic hypotension. Falls from OH lead to 30% of all hip fractures in seniors. Hospital stays from these falls cost over $30 billion a year. But here’s the hopeful part: we know how to fix this. The American Geriatrics Society’s 2023 Beers Criteria now explicitly warns against alpha blockers and certain beta-blockers in older adults. And prescriptions for ARBs and ACE inhibitors in seniors jumped from 32% to 38% between 2020 and 2023-not because they’re cheaper, but because they’re safer.The future is coming fast. Two new drugs in Phase II trials are designed to lower blood pressure only when you’re lying down, and stay neutral when you stand. Imagine a pill that protects your heart without making you dizzy. That’s not sci-fi-it’s on the horizon.
For now, the best advice is simple: don’t fear treating high blood pressure. Fear the wrong pills. Work with your doctor. Switch to safer drugs. Move slowly. Drink water. Measure your pressure properly. These steps don’t just prevent falls-they protect your heart, your independence, and your life.
Can you have orthostatic hypotension without high blood pressure?
Yes. Orthostatic hypotension can occur in people with normal or even low blood pressure. It’s caused by the body’s inability to adjust blood flow when standing, not by high blood pressure itself. Conditions like Parkinson’s, diabetes, dehydration, or certain nerve disorders can trigger it. But in older adults, it most often appears alongside untreated or poorly managed hypertension, especially when certain medications are involved.
Should I stop my blood pressure medication if I feel dizzy when standing?
No-not without talking to your doctor. Stopping medication suddenly can cause dangerous spikes in blood pressure, increasing your risk of stroke or heart attack. Dizziness is a signal to review your meds, not quit them. Your doctor can switch you to a safer drug, adjust the dose, or recommend non-drug strategies. Never make changes on your own.
Are ARBs and ACE inhibitors really safer for seniors with dizziness?
Yes. Multiple studies show ARBs and ACE inhibitors carry the lowest risk of causing orthostatic hypotension. In fact, some research suggests they may reduce OH episodes by 14-15% compared to other classes. They work by relaxing blood vessels without causing sudden drops in pressure. For older adults, especially those with diabetes or kidney issues, they’re often the preferred first choice.
How long does it take to see improvement after switching blood pressure meds?
It usually takes 4-6 weeks for the body to fully adjust to a new medication. During this time, your blood pressure will stabilize in both lying and standing positions. You may notice less dizziness within 1-2 weeks if you also start non-drug strategies like slow standing and hydration. But full safety and symptom control take time-patience is key.
Is orthostatic hypotension a sign of something worse?
Sometimes. While often caused by medications or aging, persistent OH can signal underlying issues like autonomic nervous system disorders, heart failure, or severe dehydration. If dizziness is frequent, happens without standing, or is accompanied by chest pain, shortness of breath, or fainting, see your doctor. Blood tests, EKGs, and tilt-table tests can help rule out serious causes.
Comments
Sabrina Sanches March 14, 2026 AT 16:18
I was so dizzy every morning I thought I was dying. Then my doc switched me from doxazosin to losartan and now I can get out of bed without holding onto the wall. Water before standing. Slow. Just slow. Game changer.
Katherine Rodriguez March 15, 2026 AT 20:24
This whole post is just pharma propaganda. They want you on pills forever. My grandpa stopped all his meds and his BP stabilized. He's 82 and walks 5 miles a day. No drugs needed.
douglas martinez March 16, 2026 AT 11:24
I appreciate the data-driven approach here. The SPRINT trial findings are critical and often misunderstood. Aggressive BP control doesn't cause orthostatic hypotension-poor drug selection does. The shift toward ACEi/ARBs in geriatric care is one of the most evidence-based changes in recent years. We need more clinicians to adopt this mindset.
Devin Ersoy March 16, 2026 AT 11:25
Wow. So we're just supposed to trust the same doctors who gave us opioids for back pain and statins for cholesterol numbers that don't even correlate with heart attacks? This feels like a slick marketing pamphlet disguised as medicine. I'd rather drink pickle juice and stand on my head than take another pill from this playbook.
Shruti Chaturvedi March 18, 2026 AT 01:44
My mom was on a beta blocker and kept falling. We switched to ramipril. No more dizziness. Also started drinking water before standing. Simple. Free. Works. You don't need fancy meds. Just listen to your body. And maybe don't rush to the bathroom at 3am.
Adam M March 18, 2026 AT 23:12
Alpha blockers bad. ARBs good. Switch. Done.
Dylan Patrick March 20, 2026 AT 08:03
I've been telling my patients this for years. You think you're helping by lowering BP to 120? Maybe. But if you're giving them terazosin to do it? You're setting them up for a hip fracture. I had a 79-year-old woman who fell three times in six months. Switched her to valsartan, added compression socks, told her to sit on the edge of the bed for a full minute. Six weeks later? She took her grandkid to Disney. No more hospital visits. No more fear. Just life. That's what we're fighting for.
Scott Smith March 21, 2026 AT 21:05
The real tragedy isn't the dizziness. It's how long we wait to fix it. I've seen people on dangerous meds for years because no one asked them how they felt when they stood up. Just check the number. That's not care. That's negligence. Start asking. Start listening. The answers are right there.