Liver Disease Dosing Calculator
How Liver Disease Affects Your Medications
Liver disease reduces how well your body clears medications, potentially causing dangerous side effects at normal doses.
Dose Adjustment Recommendations
When your liver is damaged, it doesn’t just affect how you feel-it changes how your body handles every pill you take. Many people assume that if a drug works for someone with a healthy liver, it will work the same way for someone with liver disease. But that’s not true. In fact, liver disease can cause drugs to build up in your system, leading to dangerous side effects-even at normal doses. This isn’t a rare issue. With over 22 million Americans living with chronic liver disease, understanding how drug metabolism changes is critical for safe treatment.
How Liver Disease Slows Down Drug Clearance
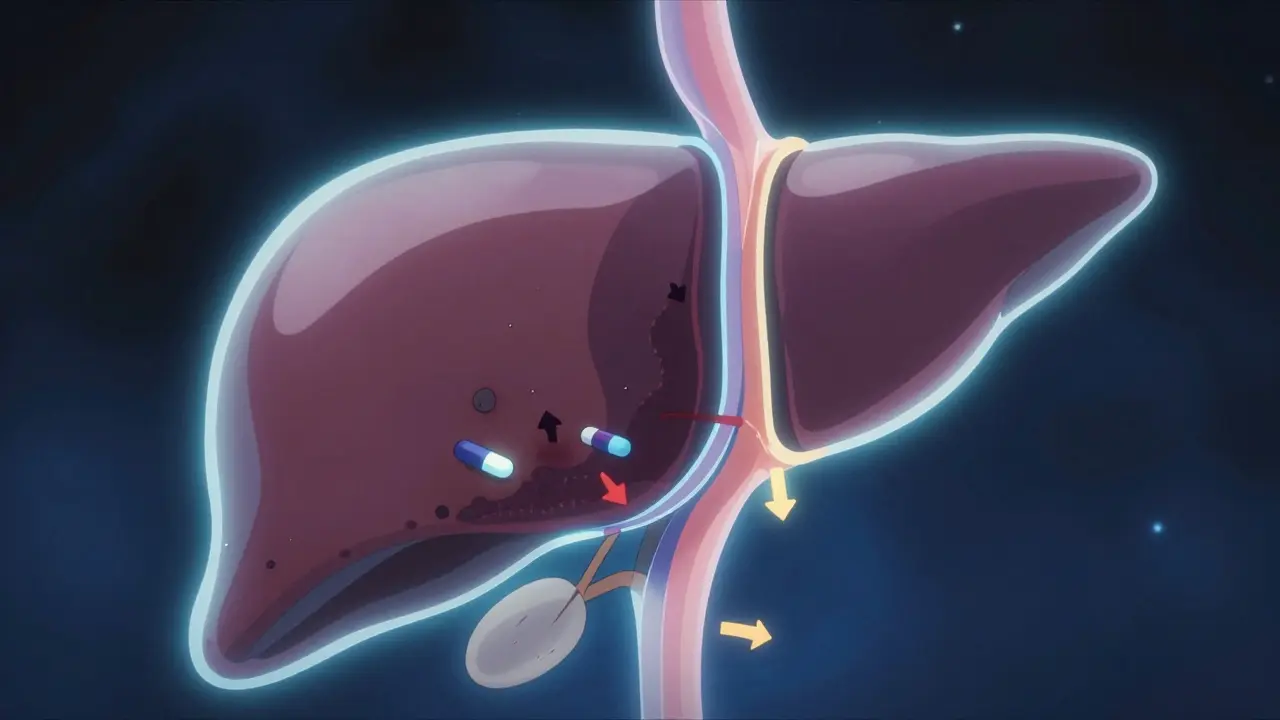
The liver doesn’t just filter toxins. It’s the main factory where drugs get broken down and cleared from your body. Two key processes handle this: metabolism (chemical changes) and excretion (removal through bile or blood). When liver disease sets in, both processes slow down. In cirrhosis, the liver’s structure changes. Scar tissue replaces healthy cells, blood flow becomes erratic, and bile ducts get blocked. Studies show that drug elimination drops by 30-50% in advanced cases. Why? Three main reasons:- Reduced blood flow: Healthy livers get about 1.5 liters of blood per minute. In cirrhosis, that drops to 0.8-1.0 L/min because of scarring and shunts that bypass the liver entirely.
- Lower enzyme activity: Key enzymes like CYP3A4 and CYP2E1-responsible for breaking down most drugs-drop by 30-60%. This means drugs stick around longer.
- Impaired transporter function: Proteins like OATP1B1 and the bile salt export pump help move drugs in and out of liver cells. In liver disease, their activity falls by 50-70%, disrupting how drugs are processed.
What’s worse? Not all drugs are affected the same way. Drugs are grouped by how easily they’re cleared. High-extraction drugs (like fentanyl or morphine) depend on liver blood flow. Low-extraction drugs (like diazepam or lorazepam) depend on enzyme activity. About 70% of commonly prescribed medications fall into the low-extraction category-meaning they’re far more likely to accumulate in liver disease.
Why Standard Doses Can Be Dangerous
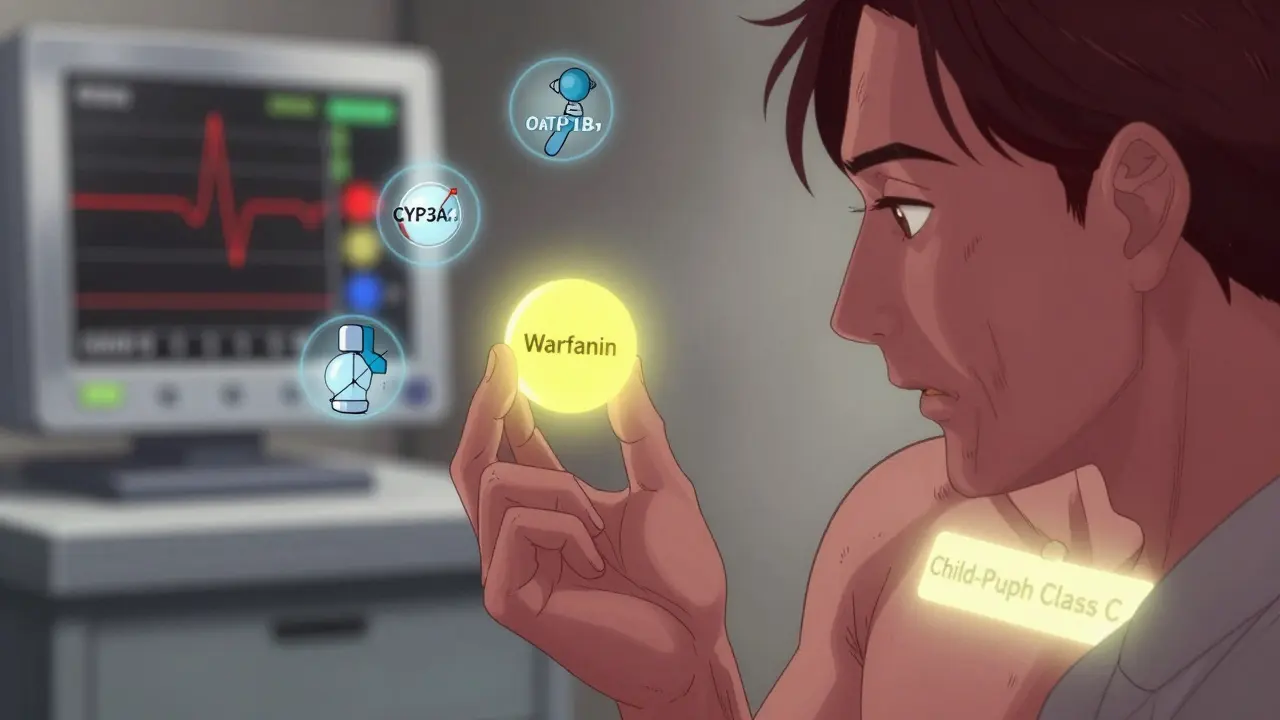
A dose that’s perfectly safe for a healthy person can be toxic to someone with liver damage. Take opioids, for example. In cirrhosis, the brain becomes more sensitive to them. Even small amounts can trigger hepatic encephalopathy-a condition that causes confusion, drowsiness, and even coma. Studies show this sensitivity increases by 30-50%. Warfarin, a blood thinner, is another example. Its clearance drops by 30-50% in cirrhosis. Without adjusting the dose, patients risk dangerous bleeding. Research from the University of Michigan found that 25-40% dose reductions are often needed just to keep INR levels stable. Even antibiotics can become risky. Ceftriaxone, often used for infections in cirrhotic patients, reaches 40-60% higher blood levels than normal because the liver can’t clear it. That’s why 68% of hepatologists report trouble with antibiotic dosing in these patients.It’s not just about toxicity. Some drugs need to be activated by the liver to work. If the liver can’t do its job, the drug might not work at all. This is especially true for prodrugs like codeine or clopidogrel. In liver disease, their active forms aren’t produced efficiently, leading to treatment failure.
How Doctors Assess Liver Function for Dosing
You can’t rely on a single blood test to judge how well someone’s liver is handling drugs. Bilirubin? Albumin? INR? All of them matter-but not on their own. The Child-Pugh score is the gold standard. It combines five factors: bilirubin, albumin, INR, ascites, and encephalopathy. It groups patients into Class A (mild), B (moderate), or C (severe). The FDA and major medical societies use this to guide dosing:- Class A: Usually no adjustment needed
- Class B: Reduce dose by 25-50%
- Class C: Reduce dose by 50-75%
Another tool gaining traction is the MELD score (Model for End-Stage Liver Disease). It’s based on bilirubin, INR, and creatinine. For every 5-point increase above 10, drug clearance drops by about 15%. This is especially useful for predicting how patients will respond to drugs with narrow therapeutic windows.
But here’s the catch: drug levels in the blood don’t always match liver test results. A patient with high bilirubin might still metabolize a drug normally. Another with normal labs might have severe enzyme damage. That’s why therapeutic drug monitoring-measuring actual drug levels in the blood-is essential for drugs like warfarin, phenytoin, or vancomycin in these patients.
What Drugs Need Special Attention?
Not all drugs are created equal when liver disease is involved. Here are key examples:- Benzodiazepines: Diazepam (with active metabolites) needs 50-70% dose reduction. Lorazepam (no active metabolites) only needs 25-40%.
- Opioids: Morphine and fentanyl require 50% or more reduction. Avoid long-acting opioids like methadone unless closely monitored.
- Antivirals: Direct-acting antivirals for hepatitis C failed in 22.7% of patients with Child-Pugh C cirrhosis when given standard doses. Adjustments cut failure rates to under 6%.
- Anticoagulants: Warfarin, rivaroxaban, and apixaban all need lower doses. INR monitoring is non-negotiable.
- Statins: Atorvastatin and simvastatin are metabolized by CYP3A4. Reduce dose by 50% or switch to pravastatin or rosuvastatin, which are less dependent on liver metabolism.
- Antidepressants: Amitriptyline and citalopram build up. Use sertraline or escitalopram at lower doses.
On the flip side, some drugs are safe. Sugammadex, used to reverse muscle relaxants during surgery, is 96% cleared by the kidneys. No dose adjustment is needed-even in severe liver disease. The same goes for most antibiotics excreted by the kidneys, like penicillin or cefazolin.
What’s Changing in Drug Development
Pharmaceutical companies are finally taking this seriously. In 2023, the FDA approved 18 new drugs with specific dosing instructions for liver disease-a 25% jump from 2022. Nearly all new drug applications now include liver impairment studies, up from 65% in 2018. The biggest shift? Physiologically based pharmacokinetic (PBPK) modeling. This isn’t guesswork. These computer models simulate how drugs move through a damaged liver using real data on blood flow, enzyme levels, and shunting. Studies show PBPK models predict drug exposure with 85-90% accuracy. The FDA’s 2024 draft guidance encourages using these models to set dosing rules. Experts predict that within five years, 70% of new drug labels will include model-based recommendations.Even more surprising? Early fatty liver-called MASLD-affects 30% of Americans. Research shows it can reduce CYP3A4 activity by 15-25% even before scarring develops. That means people with “just” fatty liver might need dose adjustments too. This changes the whole conversation: it’s not just about cirrhosis anymore.
What You Can Do
If you or someone you care for has liver disease:- Always tell your doctor about your diagnosis-even if it’s mild.
- Ask: “Is this drug processed by the liver? Do I need a lower dose?”
- Don’t assume over-the-counter meds are safe. Acetaminophen (Tylenol) is fine in small doses (≤2g/day), but higher amounts can be deadly.
- Keep track of side effects: dizziness, confusion, excessive sleepiness, or nausea could mean drug buildup.
- Ask about therapeutic drug monitoring if you’re on warfarin, seizure meds, or certain antibiotics.
Pharmacists are now playing a bigger role too. Between 2020 and 2023, pharmacist-led dose adjustment services for liver patients rose by 40%. Don’t hesitate to ask your pharmacist for help. They’re trained to spot these risks.
The bottom line: liver disease doesn’t just change how you feel-it changes how your body handles medicine. Ignoring this can lead to hospitalization, overdose, or treatment failure. But with the right knowledge, these risks are preventable.
Comments
shannon kozee March 21, 2026 AT 16:06
Really appreciate this breakdown. I work with liver patients daily and see how often standard doses cause issues. Lorazepam over diazepam? Total game changer. Simple switch, big safety win.
Pharmacists should be consulted before every new script. Too many providers still treat liver disease like it's just 'high bilirubin'.
trudale hampton March 21, 2026 AT 21:51
This is the kind of info that should be mandatory for med students. I’ve seen too many folks end up in the ER because someone just prescribed the usual dose. Liver isn’t just a ‘filter’-it’s the whole factory. And yeah, fatty liver counts too. 30% of us have it and don’t even know it.
Good job laying this out clearly.
Shaun Wakashige March 22, 2026 AT 10:27
Yikes. I just got prescribed tramadol last week. Guess I’m gonna need to call my doc. 😅
Sandy Wells March 22, 2026 AT 19:06
So we’re supposed to believe that every patient with cirrhosis needs a custom drug cocktail? This feels like overcomplicating things. Doctors already struggle with basic dosing. Now you want them to memorize enzyme kinetics and MELD scores? Good luck with that.
Most of these patients are on 10 meds already. Add one more variable and you’re asking for errors, not safety.
And don’t get me started on pharmacists 'adjusting doses'-they’re not doctors. Let them count pills, not rewrite prescriptions.
Paul Cuccurullo March 23, 2026 AT 05:21
This isn’t just medical knowledge-it’s a moral imperative. Every time we prescribe without considering liver function, we gamble with someone’s life. And for what? Convenience? Tradition? Outdated protocols?
When a patient develops hepatic encephalopathy from a simple painkiller, it’s not an accident. It’s negligence dressed up as routine.
Thank you for shining a light on this silent epidemic. The system is failing. But now we know. And knowing is the first step toward saving lives.
Solomon Kindie March 24, 2026 AT 03:38
so like if your liver is broke you just stop taking meds right? like why even have a liver if it cant do its job? why dont we just replace it with a pill that says 'i am now a liver'?
also i read somewhere that liver can regenerate so why not just wait and let it heal? why all this math? why not just chill and eat kale?
also what if your liver is kinda half dead? like 45%? is that class a b or c? who even made these categories? some phd in a basement?
Natali Shevchenko March 24, 2026 AT 06:45
It’s fascinating how we treat the liver like a broken machine when it’s actually a dynamic, adaptive organ. We don’t just reduce doses-we’re essentially trying to mimic its altered physiology with math. But the body doesn’t care about our models. It doesn’t know Child-Pugh classes. It just responds.
What if we stopped trying to calculate every variable and instead focused on listening? On monitoring symptoms? On trusting the patient’s feedback more than the lab numbers?
Maybe the real breakthrough isn’t PBPK modeling-it’s humility. Recognizing that even our best science can’t fully capture the chaos of a living system. The liver doesn’t obey equations. It whispers. And we’ve been too loud to hear it.
Casey Tenney March 25, 2026 AT 22:44
Acetaminophen is fine in small doses? That’s it? That’s the whole takeaway? People die from Tylenol every year because they think 'small dose' means 'a few extra pills won’t hurt.'
Stop pretending this is a medical issue. It’s a public education disaster. And no, your pharmacist isn’t gonna save them.