Chronic Diarrhea: Causes, Tests and Practical Steps to Feel Better
If diarrhea lasts more than four weeks, it’s not a passing bug — it’s chronic diarrhea. That constant urgency and loose stool can wear you down, disrupt work, and hide treatable problems. This page explains the common causes, the tests doctors use, simple home steps, and when you need urgent care.
Common causes are straightforward: IBS with diarrhea (IBS-D), inflammatory bowel disease (Crohn’s or ulcerative colitis), persistent infections like C. difficile, small intestinal bacterial overgrowth (SIBO), bile acid malabsorption, celiac disease, pancreatic insufficiency, and side effects of medicines (antibiotics, metformin, laxatives). Less often, thyroid problems or tumors can be behind it.
Go to the emergency room if you have high fever, severe abdominal pain, blood in the stool, rapid, unexplained weight loss, signs of dehydration, or diarrhea that wakes you at night. Those are red flags that need fast work-up.
How doctors investigate chronic diarrhea
Expect basic tests first: stool studies for bacteria, C. difficile toxin, parasites, and fecal calprotectin (which hints at inflammation). Blood tests check for anemia, inflammation markers, thyroid function, and celiac antibodies. Breath tests can detect SIBO or lactose intolerance. If those don’t give answers, a colonoscopy with biopsies or abdominal imaging is the next step.
Do one thing before your visit: keep a stool and food diary for two weeks. Note frequency, stool type (Bristol scale), foods, recent travel, antibiotics, and medicines. That record speeds diagnosis and points to triggers.
What actually helps — treatments that work
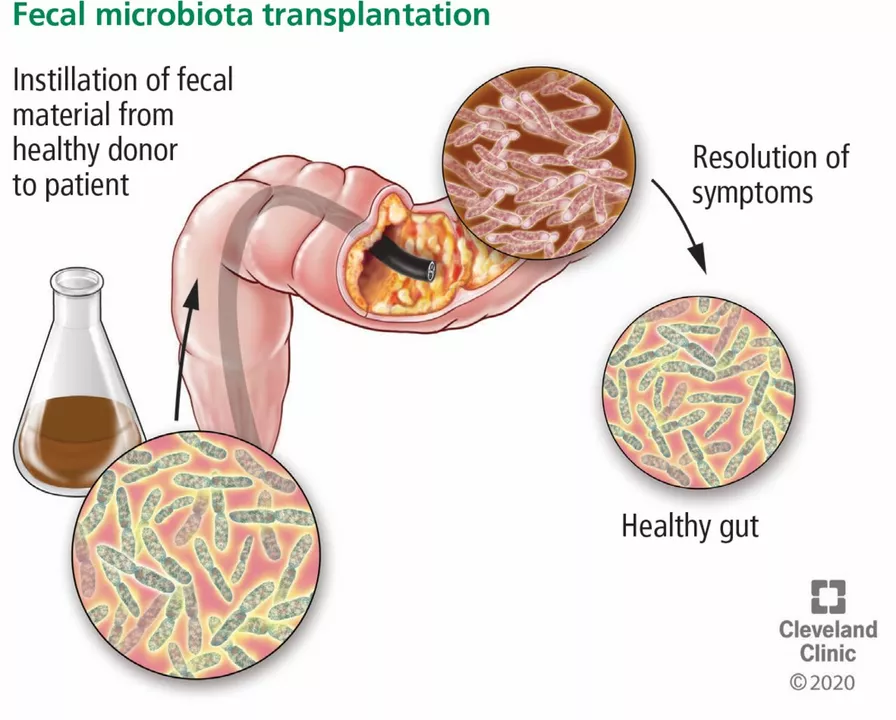
Treatment follows the cause. For IBS-D, a low-FODMAP plan, soluble fiber (psyllium), antidiarrheals like loperamide for flares, or prescription meds can help. Bile acid diarrhea often responds to bile acid sequestrants. SIBO usually needs targeted antibiotics such as rifaximin. Celiac requires a strict gluten-free diet. IBD is treated with anti-inflammatory drugs or biologics. Pancreatic enzyme replacement helps when digestion is poor.
At home, focus on hydration: use oral rehydration solutions rather than sugary sodas. Eat plain, easy-to-digest foods while you stabilize, then reintroduce fiber slowly. Probiotics (Lactobacillus strains or Saccharomyces boulardii) help some people but aren’t a guaranteed fix.
Use medicines carefully: don’t take loperamide if you have fever or bloody stools, and avoid long-term antibiotics without a doctor’s plan. Stop or switch suspect medications only after discussing with your prescriber.
Prevention and lifestyle matter: avoid unnecessary antibiotics, wash hands after travel or healthcare contact, and watch for specific food triggers. Stress can worsen bowel habits — cognitive behavioral therapy or relaxation tools can help when anxiety and symptoms are linked.
Start with a two-week food-and-stool log, stop unnecessary OTC laxatives, and book a primary care visit if problems continue. Early testing often finds treatable causes and gets you back to normal life faster. You don’t have to accept constant diarrhea — get the right tests and a clear plan.